Episode 9: [Sotos Syndrome] What If Your Child Is Unusually Large? Everything About the NSD1 Gene and Overgrowth Syndrome
“My child is a bit slow in development, but why are their height and head circumference growing so rapidly?”
Many parents naturally assume that if a child grows quickly, it simply means they have “excellent physical development” or have inherited a large build. However, if your child is exceptionally tall, has a large head, and simultaneously shows delayed neurological development compared to peers, it may not just be a matter of constitution.
Instead, it could be a sign of a genetic overgrowth syndrome. The most representative disorder among these is Sotos syndrome. First described in 1964 by the pioneering pediatric endocrinologist Dr. Juan Fernández Sotos, it has now been clearly established that the vast majority of cases are caused by abnormalities in the NSD1 gene. Today, we will explore the core clinical symptoms of Sotos syndrome, its molecular genetic mechanisms, and the latest trends in diagnosis.
📌 [Key Takeaway] Sotos Syndrome At a Glance
- Clinical Features (Phenotype): Sotos syndrome is a rare genetic disorder characterized by distinctive facial features, overgrowth (tall stature / macrocephaly), and motor and language developmental delays.
- Molecular Mechanism: The vast majority of patients carry loss-of-function variants in NSD1, a master switch gene that regulates chromatin, leading to epigenetic dysregulation.
- Diagnostic Trend: Cases confirmed through deep intronic variant reanalysis are increasing among patients who went undiagnosed by conventional protein-coding-region-focused testing.
- GEBRA-Based Data Analysis: Haploinsufficiency and domain-specific functional characteristics — both of which add complexity to variant interpretation — can be rapidly and precisely distinguished using GEBRA’s integrated workflow.
🔍The 3 Core Clinical Features of Sotos Syndrome
Sotos syndrome has a relatively distinct phenotype in clinical settings — so recognizable that clinicians often say they can suspect the diagnosis just from the face. It is broadly characterized by three key features.
1. Distinctive Facial Features
These features are most prominent during early childhood and often persist into adulthood.
- Infancy/early childhood: Wide, prominent forehead; long, narrow face; pointed chin; downslanting palpebral fissures; flushed cheeks; sparse hair at the temples.
- Adulthood: Macrocephaly, increasingly elongated face, broad and angular jaw.
2. Overgrowth
Many children are larger than average at birth, with an exceptionally rapid growth rate.
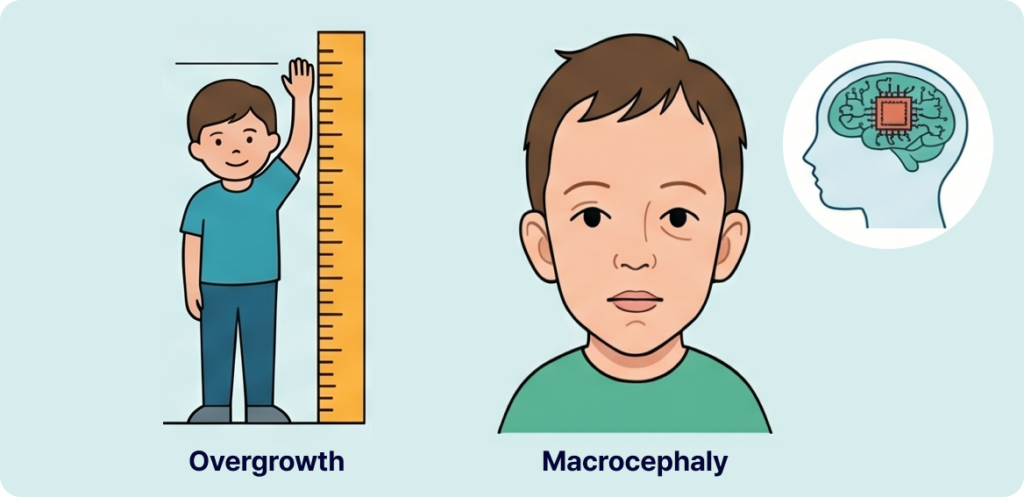
- Height and growth rate exceeding the upper end of age-matched norms.
- Macrocephaly: An unusually large head circumference is one of the most important indicators for differentiating Sotos syndrome.
3. Developmental Delays and Learning Disabilities
In stark contrast to their accelerated physical growth, neurodevelopment in these children tends to be delayed.

- Motor Developmental Delay: Delays in reaching early physical milestones such as rolling over, sitting, or walking.
- Speech & Language Delay: Significant delays in the onset of speech and language acquisition.
- Learning & Intellectual Disabilities: Although the severity varies widely and is highly individualized, general learning disabilities and intellectual impairments are frequently present.
🧬 Causative Gene NSD1 and the Epigenetic Pathogenesis
The vast majority of Sotos syndrome patients develop the condition due to pathogenic variants in the NSD1 (Nuclear Receptor Binding SET Domain Protein 1) gene, located on chromosome 5.
The Role and Importance of NSD1
NSD1 encodes a protein that regulates chromatin within cells. It acts as a “master switch,” turning on and off the expression of numerous downstream genes involved in growth and development.
- Chromatin regulator and master switch: NSD1 is an epigenetic factor that precisely regulates chromatin structure (DNA packaging) within the cell nucleus, controlling the activation of many downstream genes involved in growth and development.
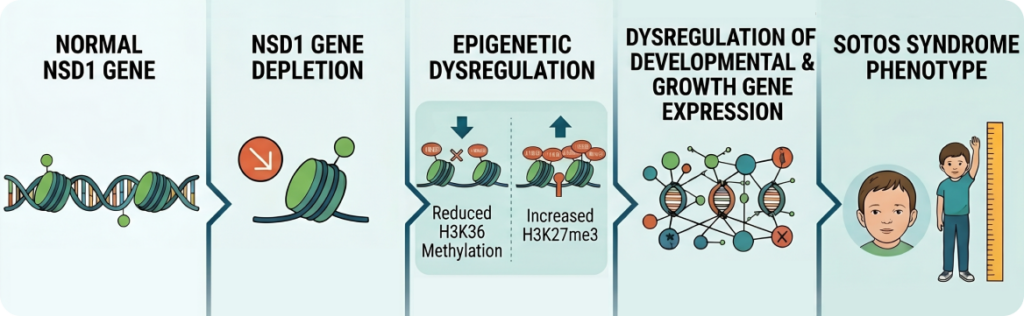
- Normal function (maintaining gene expression): Under normal conditions, NSD1 induces methylation of lysine 36 on histone H3 (H3K36). The H3K36 methylation mark suppresses PRC2 (Polycomb Repressive Complex 2) binding and H3K27me3 accumulation, helping certain genes remain in an active state.
- NSD1 loss-of-function and epigenetic dysregulation: When NSD1 function is reduced due to a gene variant, H3K36 methylation decreases. As a result, PRC2 binding and H3K27me3 accumulation increase in certain genomic regions, potentially silencing genes that should normally be active. This epigenetic dysregulation affects growth and neurodevelopmental processes, and is thought to contribute to the overgrowth and neurodevelopmental abnormalities observed in Sotos syndrome.
💡The Pathogenic Mechanism at a Glance
NSD1 reduction → Epigenetic dysregulation → Altered developmental gene expression → Sotos syndrome phenotype
📊 What Types of Variants Cause Sotos Syndrome?
NSD1 is highly sensitive to haploinsufficiency — meaning loss of function in just one allele is sufficient to cause disease. Accordingly, loss-of-function (LoF) variants that completely abolish gene function are most commonly identified.
- Common LoF variant types: Nonsense variants, frameshift variants, canonical splice site variants, exonic deletions
- Missense variants: Tend to cluster within specific functional domains critical to the protein’s core activity
💡 Functional Characteristics by Key Protein Domain
- SET domain: The catalytic core of the NSD1 protein; directly responsible for histone methylation activity.
- SAC (SET-associated Cys-rich) domain: Maintains the structural and functional integrity of the SET domain to support normal methylation activity.
- PWWP domain: A chromatin-recognition domain that interacts with DNA and histone marks, enabling NSD1 to recognize the appropriate chromatin context and bind to target genomic regions.
Early Diagnosis and the Start of Multidisciplinary Management
Diagnosing Sotos syndrome doesn’t end with identifying an NSD1 variant. It requires evaluating how well the identified variant correlates with the patient’s clinical presentation, reviewing the latest literature and disease evidence, and — when necessary — pursuing reanalysis.
GEBRA is designed to support this entire process within a single workflow, enabling clinical geneticists and researchers to perform faster and more consistent variant interpretation.
FAQ
Q1. If my child is tall and has a large head, does it mean they have Sotos syndrome?
A. Not necessarily. It could simply be familial tall stature or benign macrocephaly inherited from parents. However, if the physical overgrowth is accompanied by motor delays (like late walking), speech delays, or the distinctive facial traits mentioned above, consulting a clinical geneticist for an evaluation is highly recommended.
Q2. Is Sotos syndrome inherited from parents?
A. In the vast majority of cases, Sotos syndrome is not inherited. It typically occurs as a de novo mutation—an accidental genetic change that happens spontaneously in the egg, sperm, or early embryo. Because the parents are genetically normal, the recurrence risk for future siblings is extremely low. Family testing can easily confirm this.
Q3. What exactly does the NSD1 gene do in our body?
A. The NSD1 gene acts as a chromatin regulator and master switch (coactivator). It controls when other genes related to growth and brain development should be turned on or off. When NSD1 undergoes a loss-of-function mutation, this control mechanism breaks down, leading to unregulated physical overgrowth and developmental challenges.
Q4. A previous genetic test showed ‘no abnormalities,’ should we test again?
A. Yes, if the symptoms strongly align with Sotos syndrome. Older tests often evaluated only the protein-coding regions. Requesting a data re-analysis using the latest pipelines or upgrading to Whole Genome Sequencing (WGS) can reveal hidden causes, such as deep intronic variants, which are invisible to older testing methods.
References
Ocansey S, Tatton-Brown K, Cole TRP, et al. Sotos Syndrome. GeneReviews®. Seattle (WA): University of Washington, Seattle; 1993–2025.
Tatton-Brown K, Rahman N. The NSD1 and EZH2 overgrowth genes, similarities and differences in their associated overgrowth syndromes. Genet Med. 2007;9(4):230–236. doi:10.1097/GIM.0b013e318042d91c.