How Mobile Elements Cause Rare Disease — and How 3billion’s FindME Finds Them
At a glance
Mobile Element Insertions (MEIs) occur when DNA sequences copy and paste themselves into new genomic locations, disrupting gene function. More than 120 genetic diseases — including hemophilia, Duchenne muscular dystrophy, and neurofibromatosis — are linked to MEI. The existing standard tool, MELT, is no longer maintained and suffers from slow processing speeds. To address this, 3billion developed FindME, an in-house MEI detection tool that runs ~4× faster than MELT, achieves 5% higher Recall, and has successfully detected clinically significant variants missed by existing pipelines.
1. What are Mobile Elements?
The human genome may seem like a fixed archive of information, but hidden within it are special DNA sequences capable of copying themselves and inserting into new locations. These are called Mobile Elements (MEs).
Mobile Elements operate via a “copy-and-paste” mechanism: using an RNA intermediate, they duplicate their sequence and insert the copy into a new position in the genome. Each such event is called a Mobile Element Insertion (MEI).
There are four families of Mobile Elements known to remain active in the human genome today:
- LINE-1 (L1): The only autonomous ME — it encodes its own machinery for movement and makes up approximately 17% of the human genome. It also facilitates the movement of other ME families.
- Alu: The most abundant ME, comprising roughly 11% of the genome. Around 300 bp in length, Alu elements rely on LINE-1 machinery to retrotranspose.
- SVA (SINE-VNTR-Alu): The youngest ME family, making up approximately 0.2% of the genome. Found exclusively in humans and great apes.
- HERV-K (Human Endogenous Retrovirus K): The remnant of an ancient retroviral infection of the germline, making up roughly 0.1% of the genome. Full-length elements are about 9.5 kb, flanked by LTRs.
Research estimates that 1 in every 12–14 live human births carries a new de novo MEI — meaning these insertions are not ancient history, but an ongoing source of genomic variation in living populations.
2. Rare conditions caused by MEI
When a Mobile Element inserts into — or near — a critical gene, the consequences can be severe. To date, more than 120 pathogenic MEI variants have been documented as causes of hereditary disease.
MEIs disrupt gene function through several mechanisms:
- Direct disruption of coding sequence (exon), corrupting the resulting protein
- Aberrant splicing — disrupting normal intron/exon boundaries
- Insertion into regulatory regions — silencing transcription of the gene
Selected rare diseases caused by MEI:
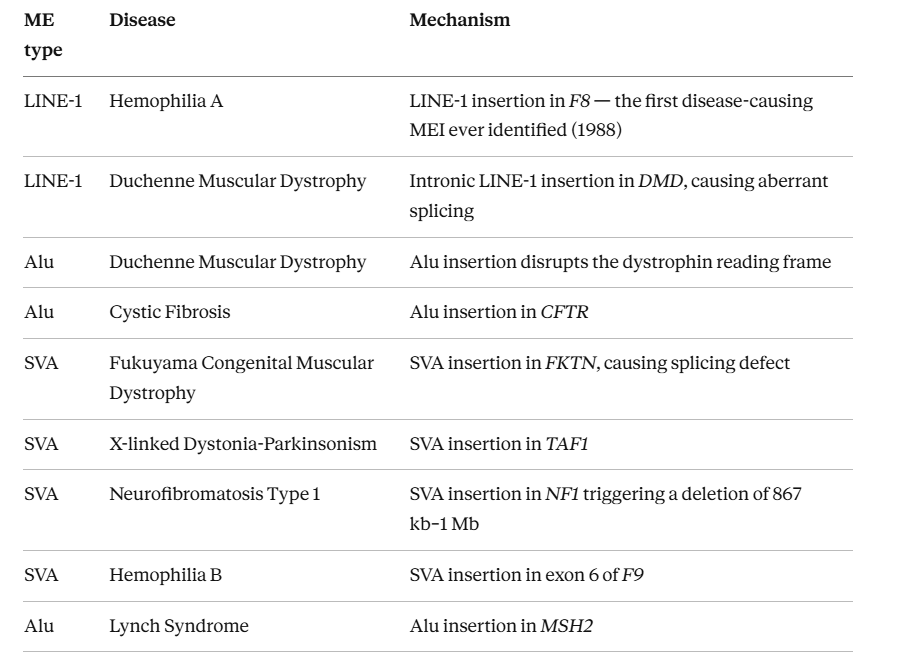
Many of these diagnoses were only made possible once MEI detection technology advanced enough to find them. Before that, they remained cases of unexplained rare disease.
3. The existing standard — MELT
Several bioinformatics tools have been developed to detect MEIs from NGS data. Among them, MELT (Mobile Element Locator Tool) has long held the status of de facto standard in the field.
MELT was originally developed as part of the 1000 Genomes Project for population-scale MEI discovery. Its ability to detect LINE-1, Alu, and SVA simultaneously from WGS data — with support for both local and cloud execution — made it the go-to tool for large-scale genomic research.
MELT’s strengths:
- Validated performance at the scale of the 1000 Genomes Project
- High precision (low false positive rate)
- Simultaneous detection of multiple ME types
However, MELT has clear limitations:
- No longer maintained: The last public update was in 2020. Issues that have emerged since cannot be addressed.
- Unexplained failures: Some samples produce errors that are difficult or impossible to debug, with no clear cause.
- Slow processing speed: Certain WGS samples can take weeks to analyze — an unacceptable bottleneck in a clinical diagnostic setting.
MELT served its purpose well as a research tool. But as clinical demand for MEI detection grows, these limitations become increasingly difficult to work around.
4. Why we built it ourselves — the origin of FindME
To address these limitations head-on, 3billion’s BI Pipeline team, BI Evidence team, and SW Gebra team jointly developed FindME: an in-house MEI detection tool built from the ground up for clinical diagnostic use.
FindME = Find Mobile Element insertion
This is not simply a drop-in replacement for MELT. FindME was designed to resolve all three of MELT’s core problems while meeting the specific demands of clinical-grade analysis.
FindME analysis workflow:
- Input BAM — accepts standard BAM-format sequencing data
- Candidate Window Detection — identifies genomic regions with evidence of MEI
- Breakpoint Pairing — matches left and right breakpoints flanking each candidate insertion
- Variant Calling — determines MEI calls from the paired evidence
- Hard / Soft Filtering — applies tiered filters to retain high-confidence calls
- Output VCF — delivers results in standard VCF format
5. What makes FindME different
Processing speed: ~4× faster on average
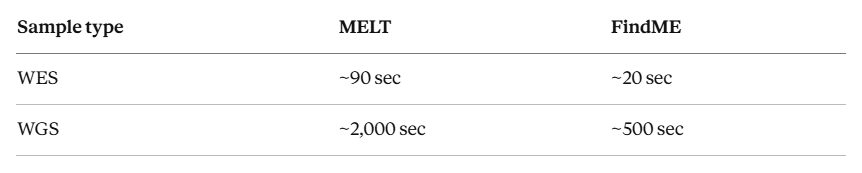
Benchmarked at 10 threads on standard samples, FindME runs 3–4× faster on average. For outlier cases that previously took MELT more than 10 days to complete, FindME finishes within 4 hours — a speedup of up to 60×.
Accuracy: F1 0.577, Recall +5%
Quantitative benchmark against the GIAB HG002 SV truth set:
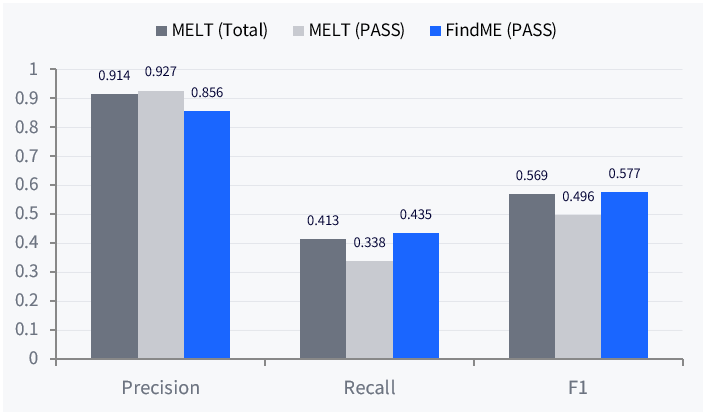
FindME’s precision is modestly lower than MELT’s, but its Recall is 5% higher — meaning it detects more true MEI variants that would otherwise be missed. In clinical diagnostics, the ability to detect rather than miss a pathogenic variant is what ultimately matters.
Maintainability and stability: in-house = immediate response
Unlike MELT, FindME is built and owned internally. When issues arise, they can be diagnosed, fixed, and redeployed immediately — without waiting on an external maintainer that no longer exists. This translates directly into pipeline stability and more reliable results for every sample submitted.
6. Clinical validation — 100% reproducibility and a case MELT missed
Confirmed MEI variant reproduction: 11/11 (100%) PASS
FindME was tested against 11 MEI variants previously confirmed in clinical diagnostic reports at 3billion. All 11 were successfully reproduced with a PASS call — across both homozygous and heterozygous cases, covering LINE-1 and Alu insertions.
A real clinical case: # 2817
A member of the clinical team identified a suspected MEI variant through manual inspection in IGV. When the existing pipeline was checked, neither MELT nor Manta had produced a call at that position — the variant had been silently missed.
FindME successfully detected the variant. The result was uploaded to Gebra and made available for clinical interpretation.
→ A clinically meaningful variant that the existing pipeline missed — found by FindME.
7. This is what 3billion is for
In rare disease diagnostics, “not missing a variant” is not a performance metric — it is the difference between a diagnosis and years of continued uncertainty for a patient and their family.
MEI has long been a blind spot in clinical genomics. The technical challenges and tool limitations meant that many patients reached the end of their diagnostic journey without an answer.
3billion built FindME to close that gap.
Finding your one answer in genomics — that is why 3billion built FindME, and what we will keep working toward.
Do you have a patient with unexplained findings where MEI may be a factor? If a case remains unresolved, we’re here to help.
This post draws on 3billion internal data and the following published literature.
Frequently asked questions
Q. What is a Mobile Element Insertion (MEI)? An MEI occurs when a repetitive DNA sequence — such as LINE-1, Alu, or SVA — copies itself via an RNA intermediate and inserts into a new location in the genome. When this happens inside or near a functional gene, it can disrupt gene expression and cause disease.
Q. Which rare diseases are caused by MEI? Over 120 pathogenic MEI variants have been documented. Associated conditions include Hemophilia A and B, Duchenne Muscular Dystrophy, Cystic Fibrosis, Neurofibromatosis Type 1, Fukuyama Congenital Muscular Dystrophy, X-linked Dystonia-Parkinsonism, and Lynch Syndrome, among others.
Q. What are the limitations of MELT, the existing standard tool? MELT has not been updated since 2020, leaving known issues unresolvable. It also produces unexplained failures in some samples that are difficult to debug, and can take weeks to process large WGS samples — a significant bottleneck in clinical settings.
Q. How does FindME perform compared to MELT? Benchmarked against the GIAB HG002 SV truth set, FindME achieves an F1 score of 0.577 (vs. MELT’s 0.569) and a Recall of 0.435 (vs. MELT’s 0.413, a +5% improvement). Processing speed averages 3–4× faster on standard samples, with up to 60× acceleration on large outlier cases.
Q. Has FindME been validated in a clinical setting? Yes. FindME reproduced 11/11 (100%) of previously confirmed MEI variants from clinical diagnostic reports. It also successfully detected a pathogenic variant that both MELT and Manta failed to call in a real clinical case (# 2817).
References
- Gardner et al. (2017). The Mobile Element Locator Tool (MELT). Genome Research. https://pmc.ncbi.nlm.nih.gov/articles/PMC5668948/
- Batcher et al. (2020). Mobile element insertion detection in 89,874 clinical exomes. Genetics in Medicine. https://www.nature.com/articles/s41436-020-0749-x
- Hancks & Kazazian (2016). Roles for retrotransposon insertions in human disease. Mobile DNA. https://link.springer.com/article/10.1186/s13100-016-0065-9
- Holste et al. (2023). Mobile element insertions in rare diseases: a comparative benchmark and reanalysis of 60,000 exome samples. European Journal of Human Genetics. https://www.nature.com/articles/s41431-023-01478-7
- Jeong et al. (2021). SVA retrotransposon insertion in MMR genes results in aberrant RNA splicing and causes Lynch syndrome. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8115629/
Get exclusive rare disease updates
from 3billion.

Sookjin Lee
Expert in integrating cutting-edge genomic healthcare technologies with market needs. With 15+ years of experience, driving impactful changes in global healthcare.