Fragile X Syndrome: The FMR1 Mutation Hidden Behind Autism and Intellectual Disability
📍Key Takeaways
- Fragile X Syndrome (FXS) is the most common single-gene cause of inherited intellectual disability, affecting approximately 1 in 4,000 ~ 1 in 7,000 males and 1 in 8,000 ~ 1 in 11,000 females.
- The clinical impact of FMR1 CGG repeat expansions differs fundamentally between Full Mutation (≥200 repeats) and Premutation (55–199 repeats)—both are clinically significant.
- Premutation carriers face risks of FXTAS (tremor/ataxia) and FXPOI (primary ovarian insufficiency), making FMR1 testing relevant beyond the proband.
Fragile X Syndrome (FXS) is a genetic disorder characterized by intellectual disability and features of autism spectrum disorder. It is the most common single-gene cause of inherited intellectual disability, and it carries an average diagnostic delay of several years from initial clinical concern.
1. FMR1 and CGG Repeat Expansion — How Full Mutation and Premutation Differ
FXS results from abnormal repetitive expansion of the CGG sequence in the regulatory region (5’UTR) of the FMR1 gene on the X chromosome. The clinical significance varies by repeat count.
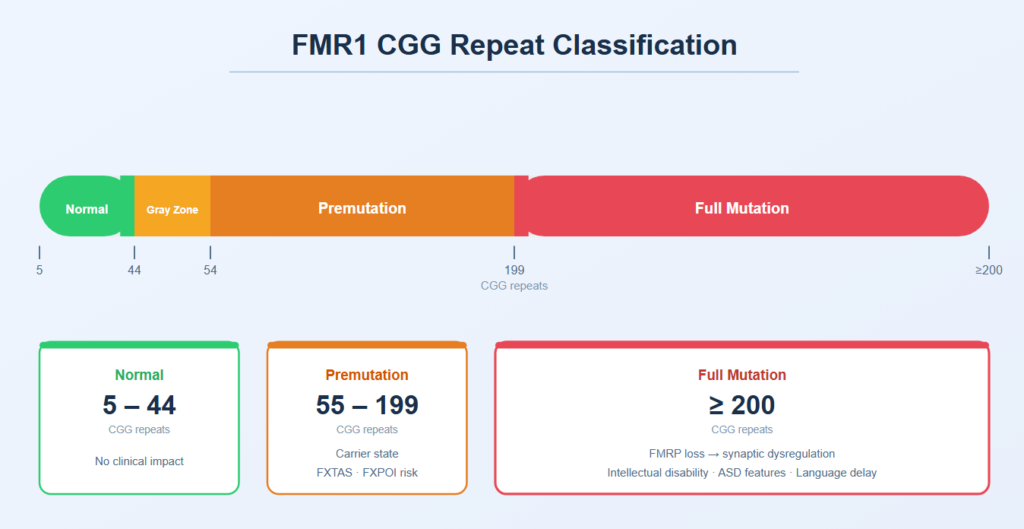
In Full Mutation, hypermethylation of the CGG repeat region silences FMR1 transcription, abolishing FMRP production. FMRP normally regulates synaptic plasticity; its absence disrupts dendritic spine maturation and underlies the characteristic cognitive and behavioral profile—intellectual disability, language delay, attention deficits, and autism-like behaviors.
2. Misidentified as Autism or ADHD — The Causes of Diagnostic Delay
Over 60% of males with FXS meet diagnostic criteria for autism spectrum disorder (ASD). Conversely, FXS accounts for approximately 2–3% of males with an ASD diagnosis. These figures highlight the clinical relevance of FXS screening within the ASD population.
The average time to confirmed FXS diagnosis is reported at 3–4 years, driven largely by the delay between initial clinical suspicion and genetic testing referral. The following combinations of features should prompt inclusion of FXS in the differential:
- Intellectual disability or developmental delay with prominent language delay
- Social anxiety, gaze avoidance, repetitive behaviors
- In post-pubertal males: macroorchidism, elongated face, prominent ears
- Family history of unexplained intellectual disability, FXTAS, or premature menopause
3. Why Premutation Carriers Matter
Premutation (55–199 CGG) does not directly cause FXS, but it carries significant clinical risks for the carrier.
FXTAS (Fragile X-Associated Tremor/Ataxia Syndrome) Primarily affects male Premutation carriers after age 50, presenting with intention tremor, cerebellar ataxia, and cognitive decline. Approximately 40% of male Premutation carriers over age 55 are affected. It is frequently misdiagnosed as essential tremor or Parkinson’s disease before genetic testing identifies the underlying cause.
FXPOI (Fragile X-Associated Primary Ovarian Insufficiency) Affects approximately 20% of female Premutation carriers, representing a roughly 13-fold increased risk compared to the general population. In any patient presenting with premature ovarian insufficiency of unclear etiology, FMR1 repeat analysis warrants consideration.
4. What Genetic Testing Can — and Cannot — Tell You
Confirmatory FXS diagnosis requires PCR-based CGG repeat sizing or Southern blot analysis. Standard whole exome sequencing (WES) does not reliably detect repeat expansions and should not be used as the primary test when FXS is the leading clinical concern.
That said, WES and comprehensive gene panels remain valuable in the broader workup of intellectual disability and developmental delay — particularly for identifying comorbid variants, ruling out phenotypically similar conditions (Angelman syndrome, Phelan-McDermid syndrome), and informing cascade testing after a proband is identified.
The average diagnostic delay for FXS is 3–4 years. If you’re investigating the cause of developmental delay or intellectual disability, genetic testing may be the right place to start. Contact 3billion’s consultation team to learn about testing timelines, costs, and required documentation.
References
- Hagerman RJ, Berry-Kravis E, Hazlett HC, et al. Fragile X syndrome. Nat Rev Dis Primers. 2017;3:17065. https://doi.org/10.1038/nrdp.2017.65
- Meadows KL, Pettay D, Newman J, et al. Survey of the fragile X syndrome and the fragile X E syndrome in a special education needs population. Am J Med Genet. 1996;64(2):428–433. https://doi.org/10.1002/(SICI)1096-8628(19960809)64:2<428::AID-AJMG39>3.0.CO;2-F
- Sherman SL, Meadows KL, Ashley AE. Examination of factors that influence the expansion of the fragile X mutation in a sample of conceptuses from known carrier females. Am J Med Genet. 1996;64(2):256–260. https://doi.org/10.1002/(SICI)1096-8628(19960809)64:2<256::AID-AJMG4>3.0.CO;2-S
- Bourgeois JA, Coffey SM, Rivera SM, et al. A review of fragile X premutation disorders: expanding the psychiatric perspective. J Clin Psychiatry. 2009;70(6):852–862. https://doi.org/10.4088/JCP.08m04476
- CDC. Fragile X Syndrome (FXS). https://www.cdc.gov/ncbddd/fxs
Get exclusive rare disease updates
from 3billion.

Soo-jung Baek
As a marketer, I strive to empower the rare disease community by sharing meaningful insights backed by our company’s expertise.