Why a Bioinformatics Engineer Says Genetic Testing Is Alive
📍Key Takeaways
- A genetic test result isn’t a snapshot. The raw sequence data stays the same for life, but as scientific knowledge grows, a past “negative” or VUS can become today’s diagnosis.
- Reanalysis works, and the data proves it. A meta-analysis found ~10% additional diagnoses, and 3billion’s automated reanalysis has given 1,482 patients a new answer — with no new blood draw (as of June 2026).
- 3billion’s reanalysis is continuous and clinic-embedded, not batch. It updates daily and runs quietly inside the diagnostic service, not as an optional add-on.
Consider a fasting blood glucose test. A reading of 95 mg/dL tells you about your body at one specific moment: this morning. By tomorrow, that number will have changed, making today’s result practically irrelevant. Chest X-rays, blood cultures, and most standard lab tests operate on the same principle—each result is a snapshot. To get a new answer, you have to test the patient again.
Genetic testing for rare diseases breaks this rule. A genomic report isn’t a snapshot; it’s a living test. It can be re-read repeatedly, returning new answers long after the initial report was issued.
Your DNA doesn’t change. The science does.
The reason is simple: a person’s genome remains virtually unchanged throughout their lifetime. The raw data from a single sequencing run—the FASTQ, BAM, and VCF files—will be identical five years from now.
What changes is everything around it—the knowledge and tools we use for interpretation. And that knowledge moves rapidly. A variant classified as a variant of uncertain significance (VUS) last year might be reclassified as pathogenic today based on new evidence. A gene with no known disease ties yesterday can become the key to a diagnosis the moment a single new paper is published.
Therefore, a “negative” genetic test doesn’t mean there is nothing to find. It simply means we haven’t found it yet, based on today’s knowledge. The test isn’t over. It is ongoing.
Five forces that keep a genetic test evolving
An unsolved case can transform into a diagnosis for five broad reasons.
- Growing disease knowledge (Disease DB) — Hundreds of new gene–disease associations are published annually, and known genes frequently reveal new modes of inheritance (MOI). Reanalysis applies each of these advances directly to a patient’s existing data.
- Sharpening variant interpretation (Variant DB) — As databases like ClinVar and HGMD expand, variants are continuously re-graded. The reclassification of a former VUS into a diagnostic finding is the single biggest driver of new answers.
- Better algorithms — Improved bioinformatics pipelines catch what the first pass missed—such as intragenic copy-number variants (CNVs) and structural variants (SVs) below microarray resolution—extracting more value from the exact same raw data.
- An updated phenotype (HPO) — In rare diseases, symptoms often surface and sharpen over the years. A minor clinical finding added later can be the missing puzzle piece.
- New family information — When parents or siblings are tested after the initial workup, family data can resolve ambiguities that a singleton analysis never could.
This isn’t aspirational. It’s measurable.
“Worth another look someday” isn’t just a hopeful sentiment; it is a clinical finding. A meta-analysis of 29 studies demonstrated that the added diagnostic yield from reanalysis is roughly 10%, driven primarily by new scientific knowledge.1
At 3billion, our automated reanalysis has provided 1,482 patients with new answers since 2024 (as of June 2026). Cases that remain unsolved are re-run through our updated pipeline; only the handful of variants backed by genuinely new evidence is escalated to a clinical geneticist. Patients who were left undiagnosed the first time finally got their answers—without a second blood draw.

Where reanalysis actually finds answers
To understand where these new diagnoses come from, we can map 3billion’s reanalysis data against the five forces above. A timely benchmark arrived in Nature Medicine in 2026: Talos, an open-source tool from Australia’s Murdoch Children’s Research Institute, the Broad Institute, and collaborators, reanalyzed 4,735 undiagnosed individuals monthly for a roughly 5% added yield.2 (Notably, the authors cite 3billion’s own 2022 study—which lifted diagnostic yield from 38% to 41% via automated reanalysis—as prior work.3)
It is no surprise that the big picture aligns—reanalysis pipelines tend to share the same skeleton. The interesting part is the grain. Talos is batch, open-source reanalysis: it re-reads a fixed cohort, deeply, in one pass. 3billion is continuous, clinically embedded reanalysis: it follows each patient over time, folding in reclassifications, new clinical findings, and family data as they arrive.
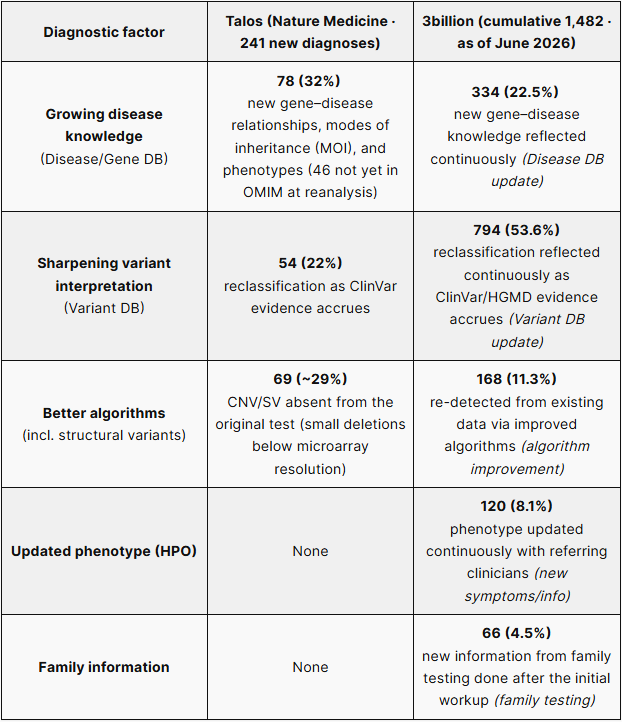
A closer look, factor by factor:
Growing disease knowledge. Both systems agree this is the single largest source of reanalysis diagnoses (Talos: 32%). The difference is tempo: where Talos refreshes monthly, 3billion refreshes daily—ahead on cadence.
Sharpening variant interpretation. ClinVar-driven reclassification is the core engine for both. 3billion goes further: beyond VUS-to-pathogenic calls, it also acts on its own AI pathogenicity score (3ASC) and splicing prediction (SpliceAI), making its reclassification signals denser.
Better algorithms. When the pipeline improves, the same raw data yields variants it couldn’t before. Structural variants are the clearest case: both tools look past single-nucleotide variants (SNVs) to CNVs, and catching the small deletions microarray misses is exactly the point.
Updated phenotype. This is where the approaches diverge. Talos relies on the clinical picture captured at the initial referral, so later symptom changes don’t register (a limitation its authors acknowledge). 3billion maintains an ongoing dialogue with referring clinicians, takes in new symptoms as they appear, updates the phenotype (HPO), and feeds it back into the next run. Staying wired into the clinic—rather than re-reading a frozen cohort—is what sets it apart.
Family information. When a parent or sibling is tested after the initial workup, questions a singleton analysis couldn’t settle can be resolved—whether a variant is de novo, or how two variants are phased. Where Talos relies on the family data available at analysis time, 3billion keeps folding newly arriving family results back into reanalysis, and into new diagnoses.
A negative result is a comma, not a full stop
For families, a negative result isn’t the end of the road. The longer a case goes unsolved, the more reanalysis shifts from being optional to essential. In one recent case, re-examining a previously negative whole-exome sequencing (WES) result finally uncovered the root cause of a lifetime of symptoms.
For clinicians, reanalysis is a matter of continuity and long-term responsibility. A genetic test shouldn’t be a one-off event; it is an ongoing process that must revisit the patient as medical science advances.
The bottom line
Reanalysis isn’t just about squeezing out a few extra percentage points of diagnostic yield. For a patient and their family, it can end a diagnostic odyssey that has lasted for years, finally opening the door to targeted treatment and care.
Genomic data isn’t a file you read once and archive. It is a living asset that can be continually questioned as science moves forward. The path forward is clear: reflect new knowledge faster, and integrate AI more deeply. The next chapter of reanalysis is just beginning.
At 3billion, reanalysis isn’t an optional add-on. It is built directly into the diagnostic service—working quietly and continuously for every patient still waiting for an answer.
Want to learn more about 3billion’s genetic testing? Or do you have a case you’re considering for reanalysis? Click the button below to submit your case, and a 3billion specialist will get back to you shortly.
References
- Dai P, et al. Recommendations for next generation sequencing data reanalysis of unsolved cases with suspected Mendelian disorders: A systematic review and meta-analysis. Genet Med. 2022;24(8):1618-1629. DOI: 10.1016/j.gim.2022.04.021
- Welland MJ, et al. Automated reanalysis of genomic data for rare disease diagnostics at scale (Talos). Nat Med. 2026. DOI: 10.1038/s41591-026-04477-5
- Seo GH, et al. Diagnostic performance of automated, streamlined, daily updated exome analysis in patients with neurodevelopmental delay. Mol Med. 2022;28:38. DOI: 10.1186/s10020-022-00464-x
Get exclusive rare disease updates
from 3billion.

Chanwoong Hwa
Bioinformatics Engineer | building in-house analysis tools and reanalysis pipelines that make genomic testing faster and more accurate for patients still waiting for answers.