Genomic Newborn Screening (gNBS) Caught 8 Cases Conventional Tests Missed — A 9,992-Newborn WGS Cohort From Qingdao
Summary
- A prospective study (Nature Health, 2026) applied WGS-based screening to 9,992 newborns in Qingdao and followed results for up to ~5 years.
- WGS flagged 268 newborns (2.7%) as positive; 19 were clinically confirmed by the follow-up date, and 8 of them had been missed by conventional screening.
- The 8 missed cases break down cleanly in the data: 6 cases of hearing loss caught by WGS alone, plus 2 cases of Wilson disease outside the scope of biochemical screening.
- WGS was not flawless: it missed 1 hearing-loss case that OAE/AABR caught. The two approaches are complementary, not hierarchical.
- The 2.7% positivity rate reflects variant-positive newborns, not affected patients. The 160 asymptomatic carriers cannot be dismissed as false positives, given late-onset and incomplete-penetrance conditions.
- Bottom line: gNBS is not a replacement for conventional NBS but a complement that fills genuine gaps in sensitivity and disease coverage.
Why this question matters
Clinicians weighing gNBS tend to ask one practical question: does WGS actually do the job biochemical screening already does — only better — or does it simply surface more variants?
A prospective cohort study published in Nature Health in June 2026 offers a fairly direct answer. Researchers performed WGS on 9,992 newborns shortly after birth and followed their outcomes for up to roughly five years, comparing the results head-to-head against conventional screening (Chen et al., Nature Health 2026).
Study at a glance
Newborns from Qingdao’s West Coast New District were enrolled within three days of birth and screened by WGS across 222 inherited diseases and 214 genes, with positive cases followed through the end of March 2025. The comparator was the standard mandatory and routine program — MS/MS for metabolic disorders, and OAE/AABR plus a four-gene panel for hearing.
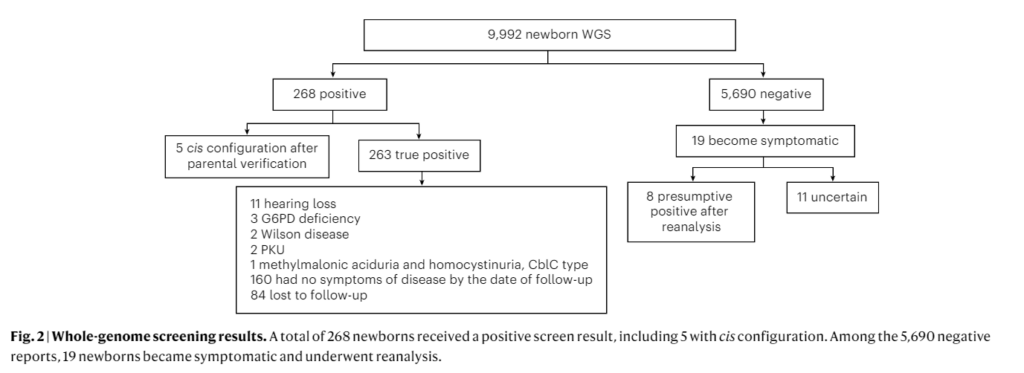
- WGS positives: 268 (2.7%) — 5 of which were resolved as cis-configuration after parental testing
- Clinically confirmed by follow-up: 19 (11 hearing loss, 3 G6PD deficiency, 2 Wilson disease, 2 PKU, 1 methylmalonic aciduria with homocystinuria, CblC type)
- 8 of the 19 had been missed by conventional screening
- Among 5,690 WGS-negative newborns, 19 became symptomatic; reanalysis identified phenotype-related variants in 8
The core finding: what the 8 missed cases actually were
This is the study’s most important point, and Figs. 2 and 3 pin down the 8 cases in the data rather than by inference.
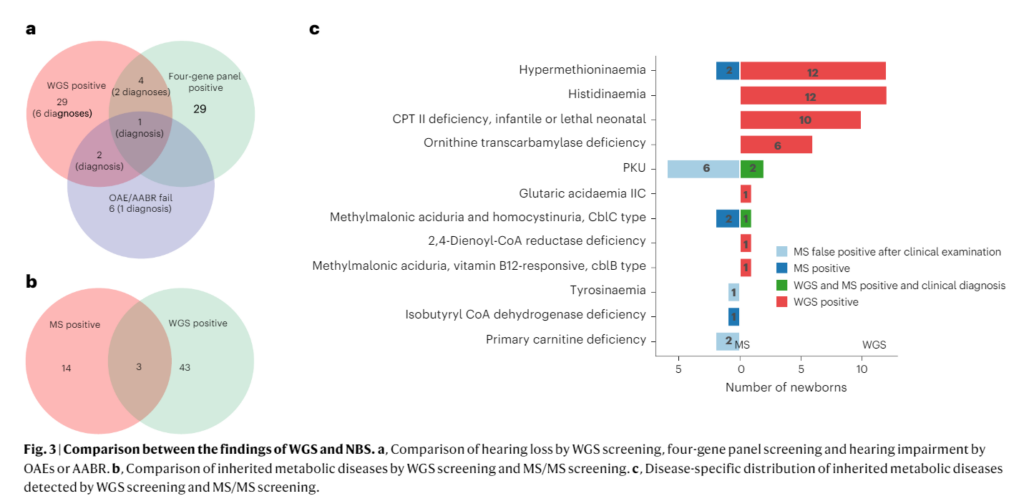
Six cases of hearing loss caught by WGS alone. In the three-way comparison of hearing screening (WGS / four-gene panel / OAE-AABR), these six newborns were flagged by none of the conventional arms — they passed the newborn physiological hearing test or carried variants absent from the panel. WGS filled that gap.
Two cases of Wilson disease. Wilson disease (ATP7B) is not part of newborn biochemical screening, so conventional methods could never have detected it.
Six plus two equals eight. The gaps gNBS closed were therefore of two kinds: hearing loss that conventional screening structurally misses (late-onset or off-panel), and disorders that biochemical screening does not address at all.
The balance cuts both ways, and that matters. In the hearing comparison, OAE/AABR caught 1 confirmed case that WGS missed. WGS is not infallible, and the two methods cover different blind spots.
What the metabolic data revealed about both methods
The confirmed metabolic disorders (2 PKU, 1 MMA with homocystinuria) were positive on both WGS and MS/MS — in this cohort, MS/MS missed no confirmed metabolic case.
What stands out instead is MS/MS false positives: 6 infants screened positive for PKU but were ruled out on clinical workup, with additional false positives in tyrosinemia and primary carnitine deficiency. This is the familiar cost of biochemical screening — unnecessary anxiety and follow-up testing for families.
How to read the 2.7%
A “2.7% positive” figure invites misreading. It is a variant-positivity rate, not a patient-detection rate. Of the 268 positives, 19 were confirmed by follow-up, 160 remained asymptomatic, and 84 were lost to follow-up.
One interpretive principle is essential here: asymptomatic does not mean false positive. Many of the conditions WGS flags are late-onset or incompletely penetrant, so a newborn symptom-free at birth may still manifest later. The authors make this explicit, noting that the observed positive predictive value likely underestimates the lifetime predictive value of WGS-based screening.
In other words, “many positives, few confirmations” is less a flaw of gNBS than an inherent interpretive challenge of applying penetrance-variable genomics in the newborn period. It is exactly why long-term follow-up and a deep phenotype–genotype database are preconditions for the approach.
The practical costs
The authors are clear that WGS carries a substantially higher per-sample cost than biochemical NBS and a longer turnaround — averaging 30 days from collection, versus three days to a week for biochemical screening, with reanalysis of symptomatic infants averaging 10 days. These are real hurdles for clinical adoption.
Conclusion: the gaps are clear, and so is gNBS’s place
What this study demonstrates is not the wholesale discovery of novel diseases, but that WGS genuinely closed gaps conventional screening leaves open. Six newborns with hearing loss who passed both the physiological test and the gene panel, and two with Wilson disease entirely outside biochemical scope — for these eight, early detection is not an abstraction. Wilson disease is a condition where early treatment changes the trajectory, and early intervention in infant hearing loss bears directly on language development.
That conventional NBS carries both false positives (6 PKU) and false negatives (6 hearing loss, 2 Wilson disease) points to gNBS as a complement with a defined role — not a replacement. The open questions — cost, turnaround, long-term follow-up of late-onset variants, and phenotype–genotype databases — are not grounds to dismiss gNBS, but the infrastructure problems to solve in order to embed it in clinical practice. The evidence already points that way.
Considering gNBS?
If gNBS is relevant to your practice, you may want to look at 3B-NEO, 3billion’s genomic newborn screening test for international clinics.
FAQ
Does gNBS replace conventional biochemical newborn screening?
No — it complements it. In this study WGS caught 8 cases that conventional hearing and biochemical screening missed, but OAE/AABR caught 1 hearing-loss case that WGS missed. The two cover different blind spots.
Which conditions would conventional methods likely have missed here?
Of the 19 confirmed cases, 8 had been missed by conventional screening: 6 hearing-loss cases identified by WGS alone, and 2 cases of Wilson disease, which is not part of newborn biochemical screening.
Does a 2.7% WGS positivity rate mean 2.7% of newborns are patients?
No. The 2.7% is the share of newborns carrying pathogenic or likely pathogenic variants (variant positivity), not a patient rate. Only 19 were clinically confirmed by follow-up; 160 remained asymptomatic.
Are the asymptomatic positives false positives?
Not necessarily. Many conditions are late-onset or incompletely penetrant, so a newborn who is asymptomatic may still develop disease later. The authors note the observed PPV may underestimate the lifetime predictive value.
What were the limits of MS/MS biochemical screening?
In this cohort MS/MS missed no confirmed metabolic case, but produced 6 false positives for PKU — driving extra testing and avoidable anxiety for families.
What are the practical barriers to adopting gNBS?
Higher per-sample cost than biochemical screening and a longer turnaround (WGS ~30 days vs. 3 days–1 week). Long-term follow-up of late-onset variants and a phenotype–genotype database are also prerequisites.
Get exclusive rare disease updates
from 3billion.

Sookjin Lee
Expert in integrating cutting-edge genomic healthcare technologies with market needs. With 15+ years of experience, driving impactful changes in global healthcare.