Why phenotypes matter for genetic testing?
You probably have heard a lot that phenotyping plays a critical role in diagnosing rare disease patients. What is phenotyping and why does it matter so much? And since it is so important, how can it be done properly to support the diagnosis?
What is phenotyping?
The term “phenotype” refers to the set of observable characteristics of an individual resulting from the interaction of its genotype with the environment.1 This can include general traits such as height, weight, hair color and also descriptions of clinical features, medical/family histories, and many others.
General traits such as height and weight are quantitative which makes it easier for physicians to input this information. However, when it comes to clinical features and other qualitative traits, it may be difficult to express them and find the right terms to explain these traits. To help professionals with these issues, the Human Phenotype Ontology (HPO) was first introduced in 2008 and has been developed over the years. The HPO provides a standardized vocabulary of phenotypic abnormalities encountered in human disease.2 It was initially for the use of computational phenotyping and precision medicines, but now it is considered as the standard form by many international organizations, clinical labs, and clinical softwares.2
This is the official website where you will find all the HPO Terms: https://hpo.jax.org/.
Why is phenotyping important in genetic testing?
Phenotyping can be essential both in the early and late stages of genetic testing. Considering the phenotypes of a patient, a physician/researcher will evaluate the patient’s condition, conduct necessary clinical tests and select the most appropriate genetic test to make a final diagnosis. Once they decide which genetic test will be performed, these phenotypes will be further utilized. First, these phenotypes will be compared to the traits of diseases, allowing geneticists to eliminate and filter any other diseases that are not relevant to the phenotypes. Second, the prioritization and the scoring system will further analyze the patient’s phenotypes and the known symptoms of a predicted disease, which leads to the final stage of diagnosis.
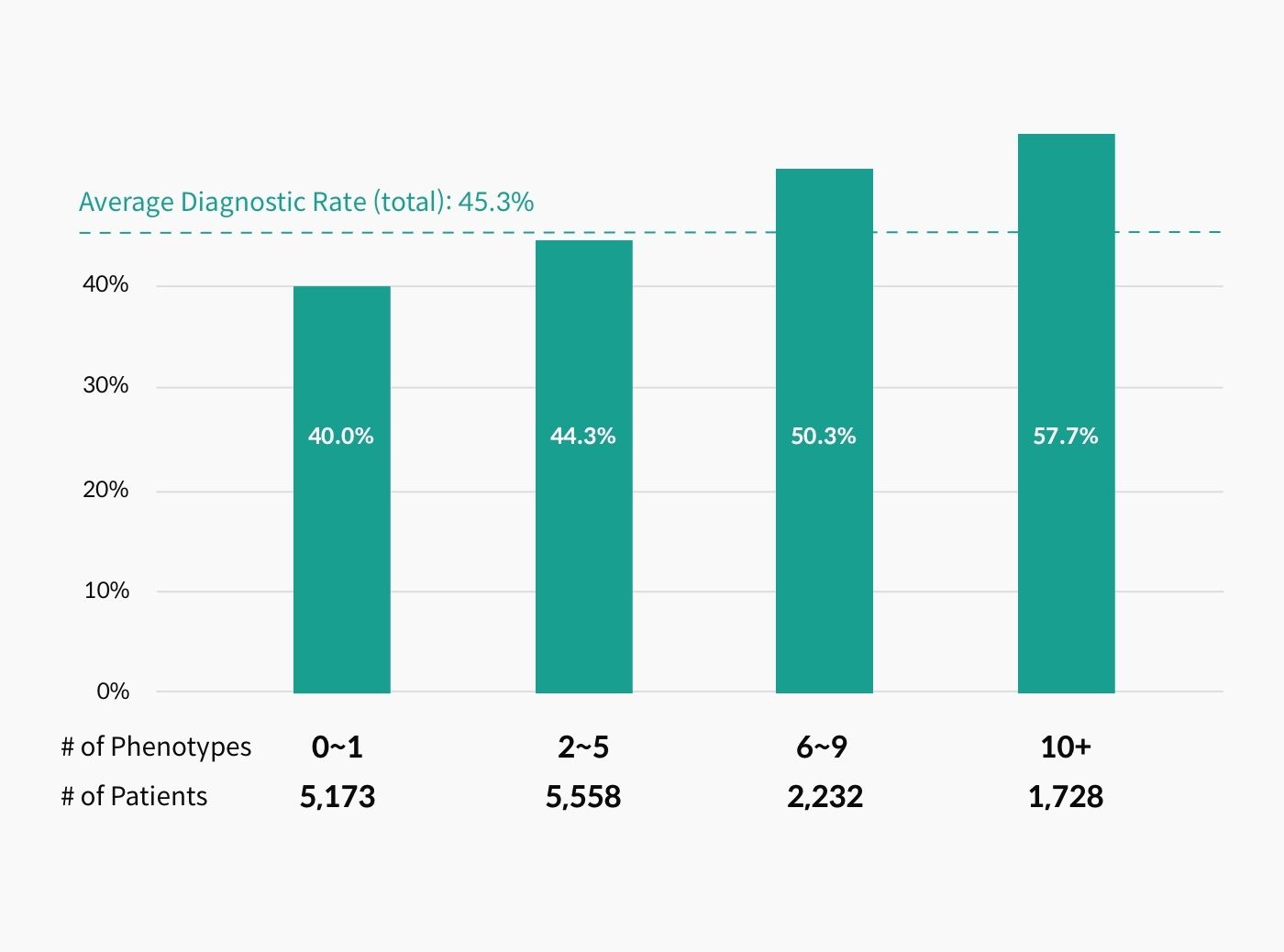
Because phenotyping is the key to diagnosis, when inaccurate phenotypes or too little information of phenotypes are provided, there is a higher possibility that the patient will be undiagnosed or misdiagnosed. In one of the recent studies, it was concluded that “any HPO-based phenotypic annotation aids variant discovery and that annotation with over five terms is recommended.3” As shown in the image below, as more phenotypes are provided, the diagnostic rate continuously increases.
Curious How We Boost Diagnostic Accuracy?
Get the newsletter every month and discover the breakthroughs with the latest reanalysis report.
Now let’s look at a real case here:
3billion received a test order for one patient with the following phenotypes: Moderate myopia, tall stature, Ischemic stroke, high arched palate, polycythemia. Through our clinical analysis, a likely pathogenic variant in one of the well-established ectodermal dysplasia related genes was found. Because the list of phenotypes did not match with this gene, the clinical report was put on hold. The clinical team wanted to learn if this patient possibly had any teeth-related phenotypes or any associated phenotypes with ectodermal dysplasia. They also wanted to make sure that there had not been any sample swapping by the ordering institution. With this information provided by 3billion, the physician re-examined the patient and found out that this patient actually had very mild teeth-related symptoms, which finally led to the final diagnosis of ectodermal dysplasia. If this additional phenotype were not provided, this patient would have been remained undiagnosed.
Any other information that can support the diagnosis?
To support the diagnosis of a rare genetic disease patient, it always helps to have more information than too little. But of course, this information must be accurate. There will be cases when some phenotypes cannot be expressed in written HPO terms. However, this information should also be addressed to support the diagnosis. For example, pictures of the patient fall into this category. Some rare disease traits can be found on the patient’s facial features. Often, the designated clinician is the only person to actually meet the patient. If the diagnostic lab/company can be provided with this information, it will certainly support the diagnosis.
Additionally, it is very important to have a family medical history. About 80% of rare disease patients have a genetic cause. Evaluating and analyzing the family’s genetic data together with the patient’s will help to increase the diagnostic rate. Most importantly, phenotypes of a patient can develop or change over time and there is new academic evidence released on a daily basis. It is very crucial to follow up on an undiagnosed patient and update his/her symptoms. When the updated phenotypes are obtained, this patient’s data must be reanalyzed and re-evaluated based on the newest information.
References
- The Department of Molecular & Comparative Pathobiology. What is phenotyping?
- Human phenotype ontology. Introduction to Human Phenotype Ontology.
- Thompson R et. al., Increasing phenotypic annotation improves the diagnostic rate of exome sequencing in a rare neuromuscular disorder. Hum Mutat. (2019).
Get exclusive rare disease updates
from 3billion.

Jane Han
Sales and business development professional in healthcare, expanding market share, managing key partnerships, and driving sales growth in the healthcare sector.





