Reproductive Genetic Carrier Screening (RGCS): When and Who to Recommend It To — A Clinical Guide from 5 Year Outcome Data
Key Takeaways
- Guidelines are shifting toward offering RGCS to everyone planning a pregnancy, not just patients with a known family history or specific ancestry.
- Making RGCS work in practice depends on the whole patient journey — from pre-visit education to long-term psychological support after results.
- Psychological outcomes differ sharply by result type: the low-chance, new increased-chance, and known-risk groups each follow a distinct course over time.
- The known-risk group — patients who already knew about their genetic risk before testing — needs a different counseling approach from the rest.
Reproductive genetic carrier screening (RGCS) is no longer reserved for patients with a specific family history or ancestry. Recent guidelines in the US, Europe, and Australia increasingly recommend offering RGCS to anyone planning a pregnancy or in early pregnancy, regardless of background.
The gap is between recommendation and practice. When to offer it, which patients to prioritize, how to explain it, and how to support patients after results — the evidence for these questions is often scattered and inconsistently applied across clinics.
Two recent papers in the European Journal of Human Genetics help close that gap:
- Paper 1 — a scoping review synthesizing 89 studies (Kraan et al., 2026), focused on how RGCS education resources should be designed
- Paper 2 — a five-year cohort study following 9,107 couples from Australia’s national RGCS program (Tutty et al., 2026), focused on what happens to patients psychologically after results
Together, they map out what’s needed across the RGCS journey — from before the test to years after the result.
A note on terminology RGCS is a population-based screening test for asymptomatic individuals, assessing genetic risk before or in early pregnancy. It is a different category of test from diagnostic testing, which is used for patients who already have symptoms or a clinical indication.
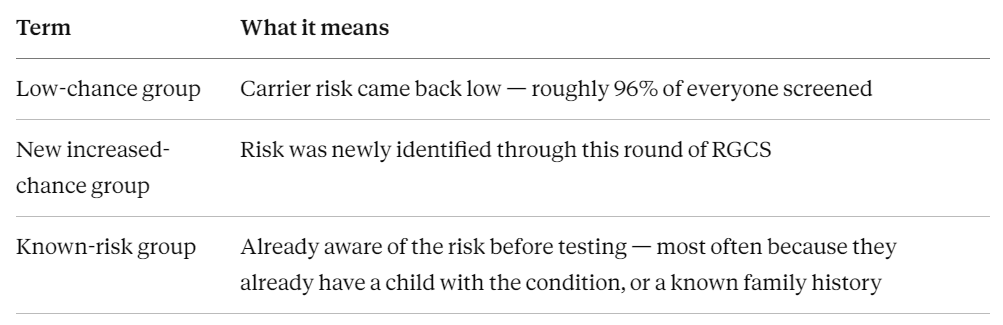
Quick reference — the three result groups discussed below
1. What RGCS Needs to Become Standard Practice
Kraan et al.’s review synthesizes 89 studies into six design principles. The points most directly relevant to day-to-day practice are below.
Timing: before the visit, not during it
Educational materials work best when patients receive them ahead of a referral or appointment, not for the first time in the exam room. Starting the conversation from zero during a visit overloads patients with information and eats into limited consultation time.
Format: narrative materials outperform chatbots and quizzes
Comics and video-based narrative formats are associated with better knowledge retention than plain text. Chatbots, podcasts, and interactive quizzes performed comparatively poorly. Tiered content — where patients can choose how much detail to engage with — helps prevent information overload.
Real-world barriers in the clinic
Support for embedding RGCS into primary care is strong, but time constraints and the burden of explaining an unfamiliar test to patients with low baseline awareness are consistently reported barriers. Notably, that burden is substantially reduced when patients arrive with some prior knowledge — which is exactly why pre-visit materials matter.
Panel size preference
Patients consistently prefer large panels over small, ancestry-restricted ones, citing reduced anxiety, greater inclusivity, and lower risk of missed findings in patients of mixed ancestry. Whether to include adult-onset genes (e.g., BRCA1/2) remains contested.
2. Which Patients Should You Recommend RGCS To
The core principle: pre-conception is the ideal window
Current guidance points toward offering RGCS to anyone planning a pregnancy or in early pregnancy — not just higher-risk groups. Within that, the evidence strongly favors the pre-conception window, since it preserves the widest range of options: natural conception, IVF, donor gametes, or adoption. RGCS can still be offered during pregnancy, but it’s worth explaining to patients that their options narrow somewhat at that point.
Testing model: sequential vs. couple-based simultaneous testing
Neither model has clear superiority in the literature, but they serve different priorities:
- Sequential testing (typically the female partner first) is preferred for the right to know one’s own result first, and for cost savings.
- Couple-based simultaneous testing is preferred for the shared experience and partner engagement it involves.
Tutty et al.’s longitudinal data adds a practical point: couple-based simultaneous testing removes the anxiety associated with waiting for a second partner’s result, since both results are reported together. This is worth mentioning when discussing testing models with patients.
The known-risk group needs a different approach
This group appears under two different labels depending on the source, though it largely describes the same patients:
- Kraan et al. refer to them as people with experiential knowledge — those who live with a genetic condition themselves, or have a close family member (a child, sibling) who has been diagnosed with one.
- Tutty et al. refer to a known increased-chance cohort — couples who already knew, before enrolling in RGCS, that they carried an increased risk. Most already had a child with the condition in question.
Because these groups overlap substantially, this article refers to them collectively as the known-risk group.
This group is broadly supportive of RGCS, but far more sensitive to how it’s discussed. In one study of cystic fibrosis families, participants explicitly said they did not want language suggesting the condition “adds meaning” to their lives. Attitudes also vary by severity and age of onset, so a standardized script is less useful here than an individualized conversation.
3. What Happens After Testing: Outcomes at Up to Five Years
Tutty et al. followed all three groups for up to five years. The trajectories are strikingly different.
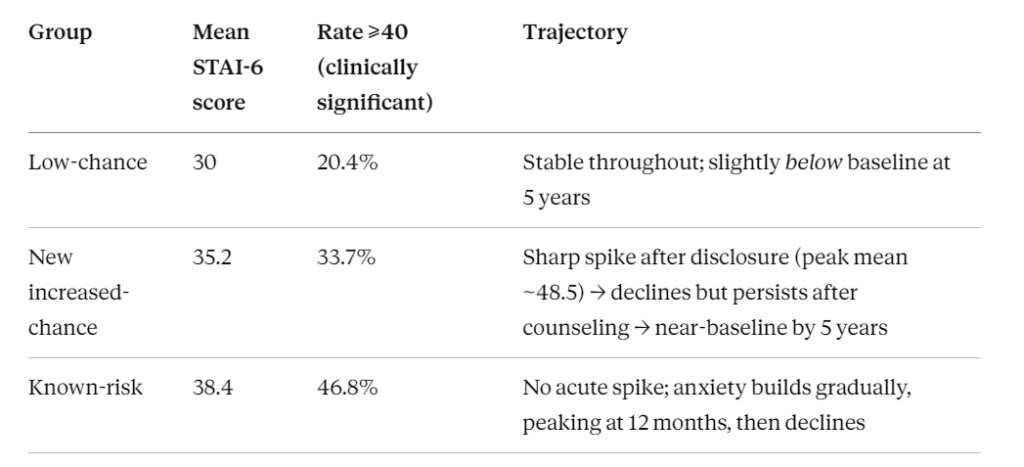
Low-chance group (96%, the majority) — the most stable outcome by far. Results provide lasting reassurance, and decision regret is minimal.
New increased-chance group — a textbook “acute shock, gradual recovery” pattern. Anxiety spikes sharply right after disclosure, begins falling after genetic counseling, and returns close to baseline by five years. This group also reports high confidence in their reproductive choices (low decisional conflict) and strong empowerment scores.
Known-risk group — a fundamentally different curve. There’s no acute spike, but anxiety accumulates gradually and peaks around 12 months before declining.
The strongest predictor of long-term anxiety at the five-year mark wasn’t the result itself — it was already having a child with a medical condition or disability. Baseline trait anxiety also predicted higher long-term anxiety, independent of the RGCS result received.
4. Counseling Considerations
- Arrange genetic counseling promptly after disclosure.
Counseling within about a week of an increased-chance result is associated with meaningful, immediate anxiety reduction. - Hold two truths at once.
Most patients recover over time — but the spike between disclosure and counseling is real and often substantial. Emphasizing only the long-term outcome, without acknowledging the acute distress, can undermine trust. - Watch the known-risk group over a longer horizon.
Their distress builds gradually rather than acutely, so check in around the 12-month mark, not just immediately after disclosure. - Choose descriptive language carefully.
Terms like “manageable” or “higher care needs” are preferable to language that implies a diminished quality of life. - Pace the information.
During emotionally sensitive periods — disclosure during pregnancy, or alongside IVF — deliver information in stages rather than all at once. - Don’t assume counseling alone resolves the distress.
Anxiety can remain elevated after the initial counseling session, which points to the need for longer-term psychosocial support structures, not a single touchpoint.
Closing Thoughts
For RGCS, the accuracy of the test itself is only part of the story. Whether it takes root in routine practice depends just as much on when it’s offered, how it’s explained, and what support follows a result.
Both studies were conducted in specific healthcare settings — Australia, the US, and Europe — where participants already had access to pre-test decision aids and genetic counseling. That context is worth keeping in mind when applying these findings elsewhere.
Sources
- Kraan, C.M. et al. (2026). Scoping review and recommendations for development and delivery of education resources for reproductive genetic carrier screening. European Journal of Human Genetics.
- Tutty, E. et al. (2026). Psychosocial outcomes of reproductive genetic carrier screening up to five years post-result. European Journal of Human Genetics.
3billion offers a Family Insight Test for known-risk families with experiential knowledge of a genetic condition, designed to clarify genetic risk before pregnancy or childbirth. Learn more at below