“Usher Syndrome Is Closer Than You Think” — A Conversation with Dr. Juan Carlos Zenteno Ruíz

📍Key Takeaways
- Early diagnosis of Usher syndrome is directly linked to treatment outcomes. An accurate diagnosis determines whether rehabilitation can begin, and marks the starting point for genetic counseling for the entire family.
- Comprehensive genetic testing is essential. Given the phenotypic variability and the existence of similar conditions, genetic testing — including WES — is the key tool for confirming a diagnosis of Usher syndrome.
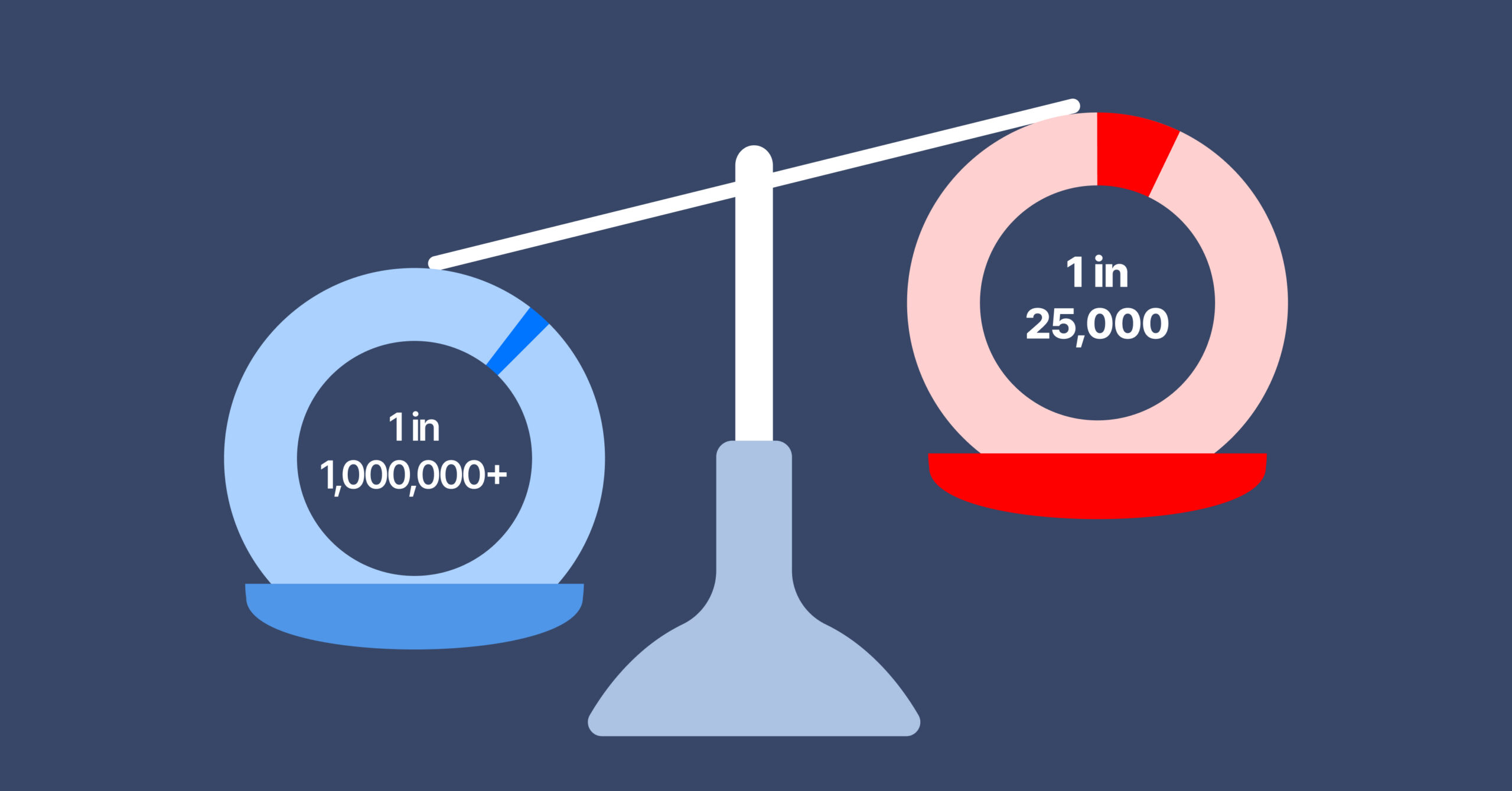
Usher syndrome is classified as a rare disease, but it is far from rare compared to most conditions in that category. While the majority of rare diseases affect approximately 1 in 1,000,000 people , the global average prevalence of Usher syndrome is estimated at approximately 1 in 25,000. This speaks to the significant role this condition plays in clinical practice.
In this post, we speak with Dr. Juan Carlos Zenteno Ruíz — a genetics specialist, Professor at UNAM’s School of Medicine, Director of the Rare Disease Diagnostic Unit (UDER), and author of more than 230 international publications — to explore the clinical reality of Usher syndrome. Drawing on his experience in the Mexican clinical setting, we examine how to suspect, diagnose, and approach genetic testing for this condition.
For Dr. Zenteno’s full profile, see the bottom of this page.
Section 1 — What Is Usher Syndrome?
Usher syndrome is an autosomal recessive genetic disorder that simultaneously causes retinal dystrophy and sensorineural hearing loss. In some subtypes, vestibular dysfunction (balance impairment) is also present.
Clinical Subtypes
Usher syndrome is classified into three main subtypes based on severity and onset:
- Type 1 (USH1): Congenital profound deafness, vestibular dysfunction from birth, and retinitis pigmentosa onset before puberty. The most severe subtype, with penetrance of 99–100%.
- Type 2 (USH2): Congenital moderate-to-severe hearing loss with normal vestibular function. Retinitis pigmentosa typically develops in adolescence. The most common subtype (approximately 60% of cases), with USH2A variants accounting for 80–90% of USH2 cases.
- Type 3 (USH3): Progressive hearing loss and retinal dystrophy, with variable vestibular involvement. More commonly reported in certain regions such as Finland.
So how does Usher syndrome actually present in clinical practice? We asked Dr. Zenteno directly.
Section 2 — Interview: Dr. Zenteno on the Clinical Frontline
Q. How often do you encounter suspected or confirmed cases of Usher syndrome in clinical practice? Also, are there specific clinical features or patterns that help you suspect Usher syndrome early in patients presenting with hearing or visual problems?
In my experience, Usher syndrome is one of the most frequent diagnoses among patients with retinal dystrophies. Since this syndrome is the most common cause of combined visual and hearing impairment, it should be suspected in any patient presenting with both retinal dystrophy and early-onset hearing loss.
Q. Why do you consider early and accurate diagnosis important in patients with suspected Usher syndrome?
Early diagnosis allows us to precisely define the diagnosis and rule out other genetic conditions that present with the combination of retinal dystrophy and hearing loss. Early recognition of the syndrome enables visual rehabilitation and hearing aid interventions, as well as accurate genetic counseling for the family. It also allows genetic counseling to begin for the family without delay.
But as critical as early diagnosis is, there are real obstacles in achieving it. We asked Dr. Zenteno about those challenges.
Q. What are the main challenges physicians face when diagnosing Usher syndrome in clinical practice?
The primary challenge is intra- and interfamilial phenotypic variability, which can lead to delays in clinical diagnosis. Furthermore, the combination of retinal dystrophy and hearing loss also occurs in other monogenic conditions, which is why a complete clinical evaluation followed by appropriate genetic testing is essential.
A Closer Look: What Drives Diagnostic Delay in Usher Syndrome
The phenotypic variability Dr. Zenteno describes is well-supported in the literature. Genetic heterogeneity is consistently cited as a key driver of diagnostic delay — the same gene can produce different phenotypes depending on the variant, and even siblings carrying identical mutations can present very differently. (Castiglione & Möller, Audiology Research, 2022. DOI)
In USH2 in particular, hearing loss may be identified in infancy, while retinitis pigmentosa may not appear until the teenage years — creating a temporal gap that, without clinical awareness of Usher syndrome, can cause the diagnostic opportunity to be missed.
Conditions that require differential diagnosis include:
- Heimler Syndrome: Profound hearing loss, retinal dystrophy, and dental anomalies.
- Bardet-Biedl Syndrome: Retinal dystrophy, obesity, polydactyly, and intellectual disability. Hearing loss is less prominent than in Usher syndrome.
- Alström Syndrome: Retinal dystrophy and hearing loss, plus multisystem involvement including obesity, diabetes, and cardiomyopathy.
- PHARC Syndrome: A very rare condition involving polyneuropathy, hearing loss, cerebellar ataxia, retinitis pigmentosa, and cataracts — differentiation from Usher syndrome is important. (Harutyunyan et al., Orphanet J Rare Dis, 2024. DOI)
- Co-occurrence of non-syndromic retinitis pigmentosa and independent hereditary hearing loss
Q. At what point in the diagnostic process should genetic testing be considered in patients with suspected Usher syndrome? Would you recommend genetic testing even before clear visual symptoms appear, in patients with hearing loss?
Genetic testing should be consideredimmediately after clinical suspicion arises and non-genetic causes of the phenotype (such as infections or medications) have been excluded. I would recommend it in cases where hearing loss is early in onset, or where family history supports a monogenic cause — such as consanguineous parents, endogamous communities, or other affected individuals in the family.
Q. In your opinion, what are the advantages of using WES (Whole Exome Sequencing)?
In my view, WES is the ideal test for patients with suspected Usher syndrome or monogenic hearing loss, as it allows analysis of all known genes associated with these phenotypes. In addition, in the case of 3billion, WES data can be periodically reanalyzed even when initial results are negative — as new causative genes may be identified, or certain variants may be reclassified as disease-causing.
If you are considering WES, contact us using the button below. Our specialists are ready to answer your questions about cost, process, and required materials.
Co-author Profile
Juan Carlos Zenteno Ruíz, MD, PhD
Dr. Juan Carlos Zenteno Ruíz earned his medical degree from the Universidad Juárez Autónoma de Tabasco, completed his specialty training in Genetics at the Hospital General de México, and holds a Master’s and PhD in Genetics from the Universidad Nacional Autónoma de México (UNAM).
He is a Professor (Profesor C de Tiempo Completo) at UNAM’s School of Medicine and a member of Mexico’s National System of Researchers (Sistema Nacional de Investigadores) at the highest level — Level 3 (2023–2032). He serves as Director of the Rare Disease Diagnostic Unit (UDER, Unidad de Diagnóstico de Enfermedades Raras) at UNAM’s School of Medicine, where he leads research into the genetic basis of rare and hereditary ocular diseases in Mexico.
To date, he has published more than 230 international articles on the genetic underpinnings of rare and hereditary eye diseases, with a cumulative citation count exceeding 5,000. He teaches both undergraduate and postgraduate courses at UNAM’s School of Medicine.
References
- Stéphanie Nguengang Wakap, Estimating cumulative point prevalence of rare diseases: analysis of the Orphanet database(2019) https://www.nature.com/articles/s41431-019-0508-0
- Mor Hanany, Comparison of Worldwide Disease Prevalence and Genetic Prevalence of Inherited Retinal Diseases and Variant Interpretation Considerations, (2024) https://perspectivesinmedicine.cshlp.org/content/14/2/a041277
Get exclusive rare disease updates
from 3billion.

Soo-jung Baek
As a marketer, I strive to empower the rare disease community by sharing meaningful insights backed by our company’s expertise.