Diagnostic Yield of WES in Infantile HCM with Normal CMA: A Case of PTPN11-associated Noonan Syndrome
1. Clinical Presentation: The Diagnostic Odyssey
A 6-month-old male presented with feeding difficulties and failure to thrive. Echocardiography revealed Hypertrophic cardiomyopathy (HP:0001639) and mild Pulmonary valve stenosis (HP:0001642). Despite a strong clinical suspicion of Noonan syndrome, initial Chromosomal Microarray (CMA) was Normal.
Instead of a “wait-and-see” approach, the clinical team opted for 3billion’s Whole Exome Sequencing (WES) to resolve the underlying genetic etiology.
2. The Diagnosis: Definitive Identification via WES
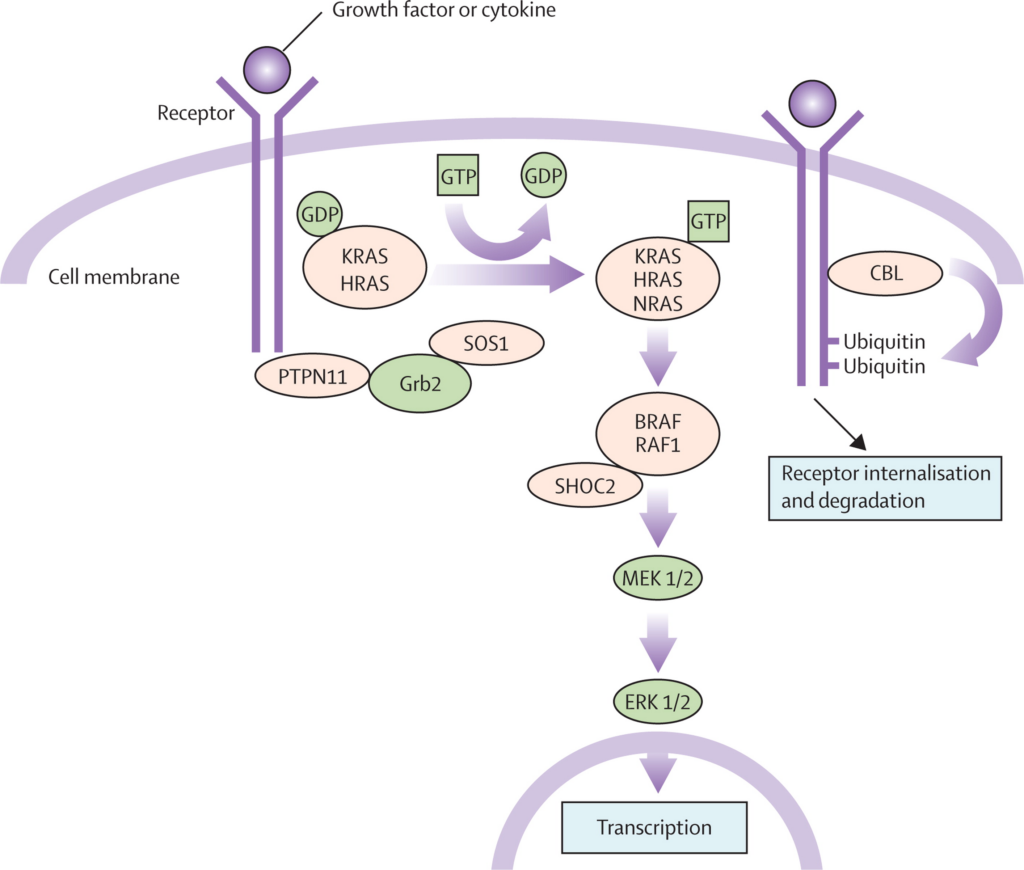
WES analysis identified a heterozygous missense variant, c.922A>G (p.Asn308Asp), in the PTPN11 gene, confirming Noonan Syndrome 1 (OMIM #163950). Subsequent cascade testing through 3billion identified the same variant in his 5-year-old brother, who exhibited mild learning disabilities but had no prior cardiac evaluation. This underscores the critical role of genomic screening in identifying at-risk relatives with variable expressivity.
3. Clinical Action: Post-Diagnostic Precision Management
Molecular confirmation mandated a shift to a specialized surveillance program:
- Hematologic Risk Assessment: Established a baseline for hematologic monitoring considering the association between PTPN11 and myeloproliferative disorders.
- Growth Hormone (GH) Calibration: Structured a monitoring protocol for GH therapy to balance growth optimization against the potential risk of accelerating myocardial hypertrophy.
- Coagulopathy Screening: Pre-operative factor analysis (e.g., Factor XI) was scheduled to mitigate hemorrhage risks during future interventions.
4. Pitfalls: The Risks of an Incomplete Diagnosis
Failure to pursue WES after a normal CMA would have resulted in:
- Iatrogenic Risks: Potential acceleration of HCM through unmonitored GH therapy.
- Familial Neglect: Leaving the sibling’s underlying risks (e.g., arrhythmia, SCD) unaddressed.
- Unforeseen Emergencies: Vulnerability to unrecognized leukemia or perioperative hemorrhages.
5. Evidence: The Clinical Imperative for WES
- Resolution Limits: CMA fails to detect SNVs/Indels that constitute >95% of Noonan syndrome cases.
- Superior Yield: In syndromic pediatric HCM, WES offers a diagnostic yield of up to 60%.
- Impact on Management: Molecular diagnosis alters clinical management in 28–52% of confirmed cases.
6. Essential Checklist for Pediatric Cardiologists
Order WES immediately if the following are present:
- CMA/Karyotyping Normal: Clear structural cardiac defects with no cytogenetic explanation.
- Extracardiac Features: Co-occurrence of dysmorphism or developmental delay.
- Infantile-onset HCM: High probability of a genetic etiology in patients <1 year.
- Family History: Unexplained early-onset heart disease or Sudden Cardiac Death (SCD).
- Conduction System Abnormalities: HCM combined with pre-excitation (WPW) or AV blocks.
[References]
- Ingles, J., et al. (2021). “Genetic Testing for Heritable Cardiovascular Diseases in Pediatric Patients: A Scientific Statement From the American Heart Association.” Circulation: Genomic and Precision Medicine. Link
- Roberts, A. E., et al. (2013). “Noonan syndrome.” The Lancet. Link
- NICUSeq Study Group. (2021). “Effect of Whole-Genome Sequencing on the Clinical Management of Acutely Ill Infants With Suspected Genetic Disease” JAMA Pediatrics. Link
Get exclusive rare disease updates
from 3billion.

Sookjin Lee
Expert in integrating cutting-edge genomic healthcare technologies with market needs. With 15+ years of experience, driving impactful changes in global healthcare.