Key to Differential Diagnosis of hEDS vs. vEDS: Limitations of the Beighton Score and the Role of Genetic Testing
Simple Flexibility or a Life-Threatening Connective Tissue Disorder?
The Diagnostic Trap — Where “Flexible” Ends and “Life-Threatening” Begins

Imagine a female patient in her 20s presenting with excessive joint laxity. She has a Beighton Score of 7, skin hyperextensibility, and a history of recurrent dislocations. At first glance, this appears consistent with hypermobile Ehlers-Danlos syndrome (hEDS). However, further history reveals that a family member died from an unexplained arterial rupture.
This scenario illustrates why differentiating Ehlers-Danlos syndrome (EDS) subtypes is not merely academic—it is a life-saving clinical decision. While hEDS is the most common subtype, vascular Ehlers-Danlos syndrome (vEDS), caused by pathogenic variants in COL3A1, carries the highest mortality risk, and the first vascular event may result in sudden death. Because clinical phenotypes overlap significantly, the Beighton Score—our most widely used clinical tool for assessing generalized joint hypermobility—cannot distinguish between these subtypes.
Part 1. Why the Beighton Score Alone Is Insufficient
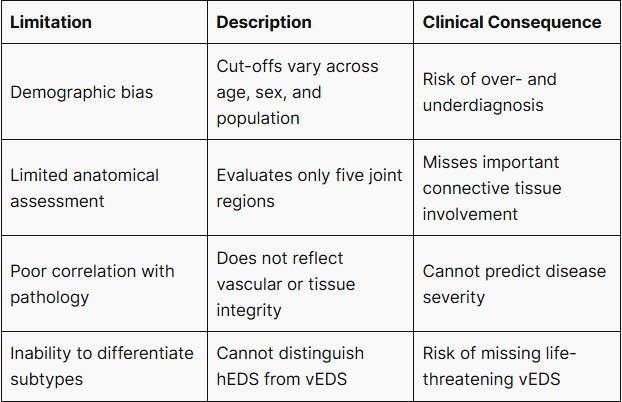
The Beighton Score is the most widely used clinical tool for assessing generalized joint hypermobility (GJH) and is incorporated into both the 1998 Brighton criteria and the 2017 International Classification of EDS. However, recent studies (2023–2025) have highlighted important limitations.
1. Demographic Bias
A 2023 review by Feldman et al. demonstrated that Beighton Score cut-offs lack consistent standardization across age, sex, and ethnicity. This introduces the risk of overdiagnosis in children, who naturally exhibit greater flexibility, and underdiagnosis in adult males and certain populations.
2. Limited Anatomical Scope
The Beighton Score evaluates only five joint regions (fifth finger extension, thumb apposition, elbow hyperextension, knee hyperextension, and trunk flexion). It does not assess the shoulders, hips, or spine, nor does it capture soft tissue pathology involving fascia and tendons—structures frequently associated with pain and dysfunction in EDS patients (Wang et al., 2025).
3. Lack of Correlation with Underlying Pathology
Studies have demonstrated limited correlation between Beighton Scores and objective measures of connective tissue integrity, including tissue structure and vascular abnormalities (Sulli et al., 2023). A high Beighton Score does not necessarily reflect the severity of collagen dysfunction. Importantly, in vEDS, life-threatening vascular events may occur even in patients with minimal or absent hypermobility.
Table 1. Summary of Beighton Score Limitations
Part 2. hEDS and vEDS — Overlapping Phenotypes, Divergent Clinical Outcomes
Substantial Phenotypic Overlap
EDS subtypes, including hEDS, classical EDS (cEDS), and vEDS, exhibit substantial clinical overlap rather than existing as completely distinct entities. Members of the same family may receive different subtype diagnoses based solely on clinical features (Rahmoune et al., 2023).
This overlap creates a significant diagnostic challenge: vEDS may remain unrecognized unless specifically considered and confirmed through genetic testing.

Pathogenic COL3A1 Variants and Vascular Fragility
vEDS is caused by pathogenic variants in the COL3A1 gene, which encodes type III collagen, a key structural component of blood vessels and hollow organs. Defective type III collagen results in marked fragility of arterial and organ walls, predisposing patients to spontaneous rupture.
Compared with other heritable aortic disorders such as Marfan syndrome or Loeys-Dietz syndrome, COL3A1 variant carriers demonstrate both the highest incidence and earliest onset of peripheral arterial events, including arterial dissection and rupture (Calderón-Martínez et al., 2025).
Part 3. Early Clinical Indicators That Should Prompt Suspicion of vEDS
Emerging evidence (2023–2025) highlights early clinical features that may facilitate earlier recognition of vEDS.
Unexplained easy bruising
This may be the earliest clinical manifestation, particularly in pediatric patients, and is often initially misattributed to hematologic causes.
Congenital musculoskeletal abnormalities
Congenital clubfoot and distal contractures have been reported more frequently in vEDS cohorts (Bowen et al., 2023).
Perinatal indicators
Preterm birth and amniotic band sequence have been proposed as potential early indicators based on observational cohort data.
Early-onset complications
Spontaneous pneumothorax, arterial events, or severe varicose veins occurring before age 40 should prompt evaluation for pathogenic variants in connective tissue genes, including COL3A1 (Sun et al., 2023).

Part 4. Clinical Impact of Delayed Diagnosis
Delayed diagnosis of vEDS carries substantial clinical risk.
Studies have reported that:
- Approximately 21% of pediatric vEDS patients experience arterial rupture or bowel perforation before age 18
- The median age of first major vascular event is 11 years, with events documented even in infancy (Wilkinson et al., 2024)
These findings underscore the critical importance of early identification through appropriate genetic evaluation.
Part 5. Genetic Testing as a Critical Clinical Tool
Impact on Clinical Management
A confirmed molecular diagnosis significantly alters patient management.
For patients with confirmed pathogenic variants in COL3A1:
Surveillance
Regular imaging of the arterial system, including CT angiography or MRI, is initiated to monitor vascular integrity.
Medical management
Preventive pharmacologic therapy, including beta-blockers, angiotensin receptor blockers, or celiprolol, may be considered.
Lifestyle modification
Patients are advised to avoid activities that increase vascular stress, such as heavy lifting or high-impact exercise.
For patients initially suspected of having hEDS, genetic testing is essential to exclude life-threatening subtypes, including vEDS and other heritable connective tissue disorders.
Advantages of NGS Panels Over Single-Gene Testing
Because clinical features overlap among connective tissue disorders such as Marfan syndrome, Loeys-Dietz syndrome, and vEDS, next-generation sequencing (NGS) panel testing provides a more efficient and comprehensive diagnostic approach.
NGS panels offer:
- Ability to identify at-risk asymptomatic family members
- Higher diagnostic yield
Greater cost-effectiveness compared with sequential single-gene testing

Part 6. Pregnancy Considerations in vEDS
Historically, pregnancy in vEDS patients was associated with significant maternal risk. However, recent evidence demonstrates improved outcomes when diagnosis is established and management is conducted at specialized centers.
A 2025 cohort study reported no fatal vascular events among 121 pregnancies managed with appropriate genetic diagnosis and multidisciplinary care (Van Den Bersselaar et al., 2025).
Genetic diagnosis enables informed risk assessment and individualized reproductive planning.
Clinical Decision Framework
The Beighton Score should be viewed as a screening tool, not a definitive diagnostic instrument.
Genetic testing should be strongly considered in patients with:
- Pregnancy planning in patients with suspected EDS
- Unexplained easy bruising
- Family history of arterial rupture or sudden death
- Early-onset vascular complications
- Unexplained pneumothorax or organ rupture
- Suspected connective tissue disorder with unclear subtype
Conclusion
Accurate differentiation between EDS subtypes has direct implications for patient survival and clinical management.
Because clinical features alone cannot reliably distinguish between subtypes, genetic testing plays a central role in confirming diagnosis, guiding surveillance, and reducing the risk of catastrophic vascular events.
Early genetic diagnosis enables proactive management and improves long-term outcomes in patients with heritable connective tissue disorders.
When clinical findings alone are insufficient to distinguish between subtypes, genetic testing provides definitive diagnostic evidence.
Consult with our genomic specialists to discuss testing suitability and interpretation strategies.
References
- Aziz Q, et al. (2025). Clinical Practice Updates: AGA Clinical Practice Update on GI Manifestations and Autonomic or Immune Dysfunction in Hypermobile Ehlers-Danlos Syndrome: Expert Review. https://doi.org/10.1016/j.cgh.2025.02.015
- Bowen JM, et al. (2023). Diagnosis and management of vascular Ehlers-Danlos syndrome: Experience of the UK national diagnostic service, Sheffield. https://doi.org/10.1038/s41431-023-01343-7
- Brancato V, et al. (2025). NGS Approaches in Clinical Diagnostics: From Workflow to Disease-Specific Applications. https://doi.org/10.3390/ijms26199597
- Calderón-Martínez E, et al. (2025). Differences in Arterial Events in Vascular Ehlers-Danlos, Loeys-Dietz, and Marfan Syndrome. https://doi.org/10.1016/j.jacc.2025.04.023
- Doolan BJ, et al. (2023). Dermatologic manifestations and diagnostic assessments of the Ehlers-Danlos syndromes: A clinical review. https://doi.org/10.1016/j.jaad.2023.01.034
- Feldman EM, et al. (2023). A narrative review of the literature on illness uncertainty in hypermobile ehlers-danlos syndrome. https://doi.org/10.1186/s12969-023-00908-6
- Hadar N, et al. (2024). Heterozygous THBS2 pathogenic variant causes Ehlers–Danlos syndrome with prominent vascular features in humans and mice. https://doi.org/10.1038/s41431-024-01559-1
- Haem E, et al. (2025). Vascular Ehlers-Danlos Syndrome and Pregnancy: A Systematic Review. https://doi.org/10.1097/01.aoa.0001125536.76136.aa
- Rahmoune H, et al. (2023). The Ehlers-Danlos syndrome, a disease of late diagnosis: report two cases. https://doi.org/10.1093/rheumatology/kead323.054
- Sulli A, et al. (2023). NAILFOLD CAPILLAROSCOPIC STATUS IN HYPERMOBILE EHLERS DANLOS SYNDROME PATIENTS: PILOT INVESTIGATION. https://doi.org/10.1136/annrheumdis-2023-eular.4886
- Sun Y, et al. (2023). Case report of a young male, with recurrent pneumothorax, hemoptysis and intrapulmonary cavitary lesions. https://doi.org/10.1097/md.0000000000035436
- Van Den Bersselaar LR, et al. (2025). Pregnancy and Delivery Outcomes in Vascular Ehlers–Danlos Syndrome: A Retrospective Multicentre Cohort Study. https://doi.org/10.1111/1471-0528.18142
- Wang J, et al. (2025). Fascial Pathophysiology in Hypermobility Spectrum Disorders and Hypermobile Ehlers–Danlos Syndrome: A Review of Emerging Evidence. https://doi.org/10.3390/ijms26125587
- Wilkinson JM, et al. (2024). Vascular Ehlers-Danlos syndrome in children: evaluating the importance of diagnosis and follow-up during childhood. https://doi.org/10.1038/s41431-024-01773-x
Get exclusive rare disease updates
from 3billion.

3billion Inc.
3billion is dedicated to creating a world where patients with rare diseases are not neglected in diagnosis and treatment.